Tutorial Script – Lecture 3: Basal Ganglia
Date: Wednesday, 29 April 2026 (archive — session already held)
Duration: 90 minutes
Lecture slides: AC_MS_3_BasalGanglia.pdf
0. Before the Tutorial (prep, not spoken)
Likely questions from students:
- “Why is the pathway called ‘direct’ if it has two inhibitory steps?”
- “How exactly does dopamine fix Parkinson’s if it acts on both pathways?”
- “What’s the difference between GPe and GPi — they sound the same?”
- “DBS stimulates but König says it actually inhibits — how does that work?”
- “Where does Huntington’s fit in — no one explained it clearly in the lecture?”
Known misconceptions to actively address:
- Thinking dopamine is always excitatory — it depends on the receptor (D1 vs. D2)
- Confusing GPe (external = part of indirect pathway) with GPi (internal = output)
- Believing “more synapses = more inhibition” — the net effect depends on the number of sign-inversions, not the absolute count
- Assuming Parkinson’s simply = “less movement” — it’s about tonic over-inhibition of the thalamus
- Mixing up Parkinson’s (hypokinesia) and Huntington’s (hyperkinesia) lesion locations
Things to look up again before tutorial:
- Exact neurotransmitter at each synapse in the direct/indirect pathway (especially the Striatum → GPi step in direct: GABA)
- Note: the lecture marks the GPi-to-thalamus projection as tonic inhibitory — this is the “gate”
- Sacks’ “Awakenings” is referenced in the slides for L-DOPA context — good hook
- MPTP story: 1976 (first case) + 1982 (drug contamination wave) → MAO-B converts MPTP to MPP+, selectively destroys SNc neurons; now the standard animal model
- Epidemiology numbers (Slide 37): 228/100K prevalence, ~15M worldwide, 275% increase 1990→2026, 80K total annual cost per patient
- Non-motor symptoms (Schapira et al. 2017, Slide 35): precede motor symptoms by 2–5 years — hyposmia, REM sleep disorder, autonomic dysfunction, depression
- L-DOPA strategy: start as late as possible to delay dyskinesia onset; co-administer Carbidopa to block peripheral conversion
- 2026 experimental treatments: Bemdaneprocel (iPSC-derived DA neurons, Phase II), GDNF gene therapy, Prasinezumab (anti-alpha-synuclein antibody)
1. Opening & Hook (5 min)
Opening question for the group:
“Imagine you want to pick up your coffee mug. How does your brain decide to execute that movement and not the 50 other things your arm could do at the same time? Who is doing the filtering?”
Let the group speculate for 2 minutes. Guide toward: the brain needs a selection mechanism, not just a movement generator. The basal ganglia are that filter.
Alternative hook (if group is quiet):
“In 1982, six people suddenly developed severe Parkinson’s disease — overnight, all of them, after using contaminated street drugs. What does that tell us about how the brain controls movement?”
(MPTP story: accidental model for Parkinson’s — dopaminergic neurons in SNc destroyed within days)
2. Link to Last Week (5 min)
Last week (Lecture 2): the cerebellum = supervised learning machine. It refines ongoing movements by comparing expected vs. actual outcomes (error-correction, climbing fiber = teacher signal). It gives inhibitory output (Purkinje cells → DCN), operates without tonic sustained activity.
Today: the basal ganglia = reinforcement learning gating system. Not the same as the cerebellum. Key contrast:
| Cerebellum | Basal Ganglia | |
|---|---|---|
| Learning type (Doya) | Supervised | Reinforcement |
| Output mode | Inhibitory, context-dependent | Tonic inhibition — always on |
| Main role | Optimize/fine-tune movement | Select/gate which movement happens |
Bridge question:
“The cerebellum is sometimes described as the brain’s ‘optimizer.’ If that’s true, what role might the basal ganglia play — and what kind of learning would you expect them to implement?“
3. BG Anatomy — The Structures (15 min)
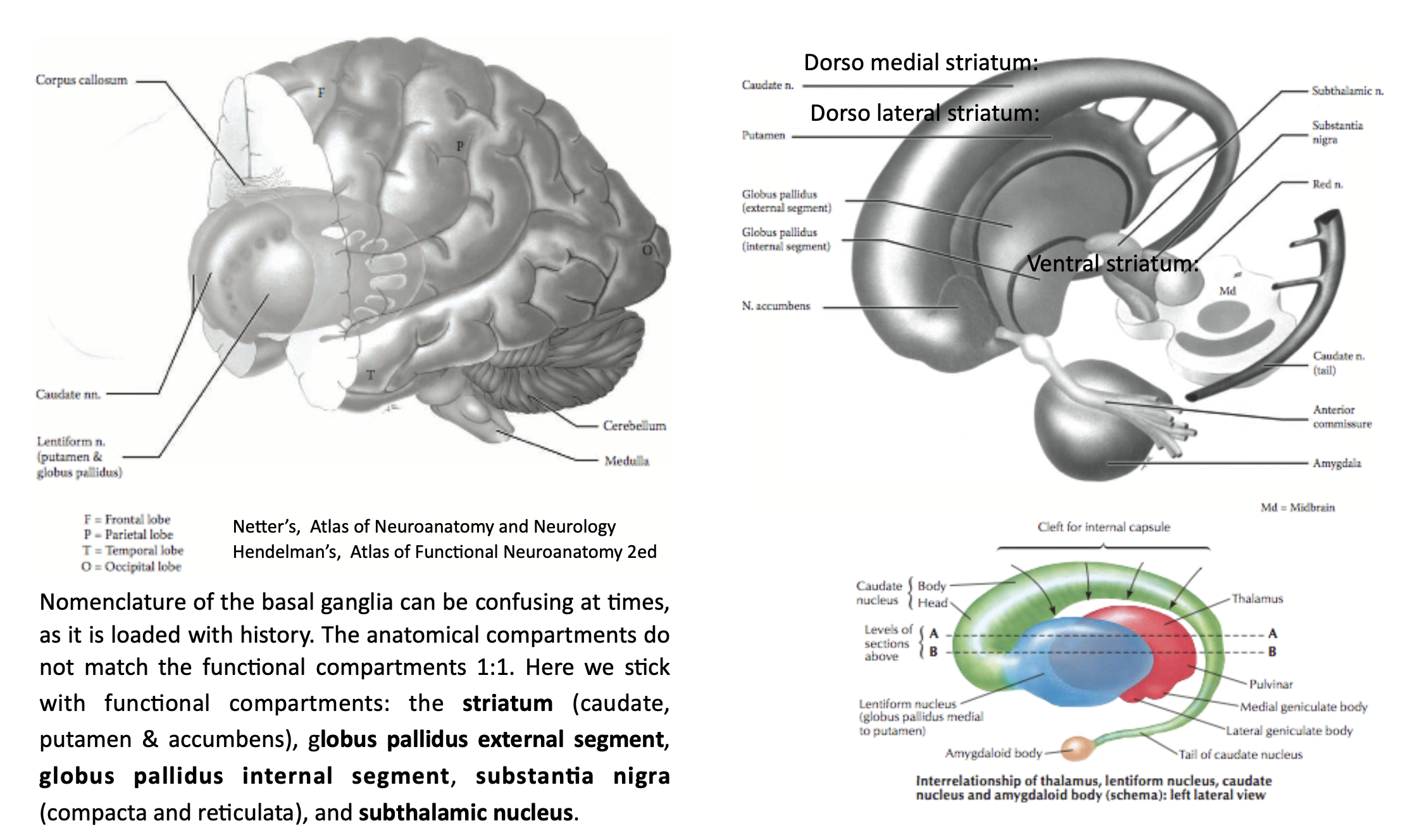
Core Message
The basal ganglia are not the cortex. Most students think “deep brain = mysterious.” But the anatomy is logical once you see the information flow: in through striatum, out through GPi/SNr, relay via thalamus back to cortex.
Terminological Trap (worth flagging explicitly)
- Normal “ganglion” = neuron cell bodies outside the CNS (e.g. dorsal root ganglia)
- “Basal ganglia” = neuron cell bodies inside the CNS — the name is a historical misnomer
- The lecture flags this explicitly: it is an inconsistency, not an error
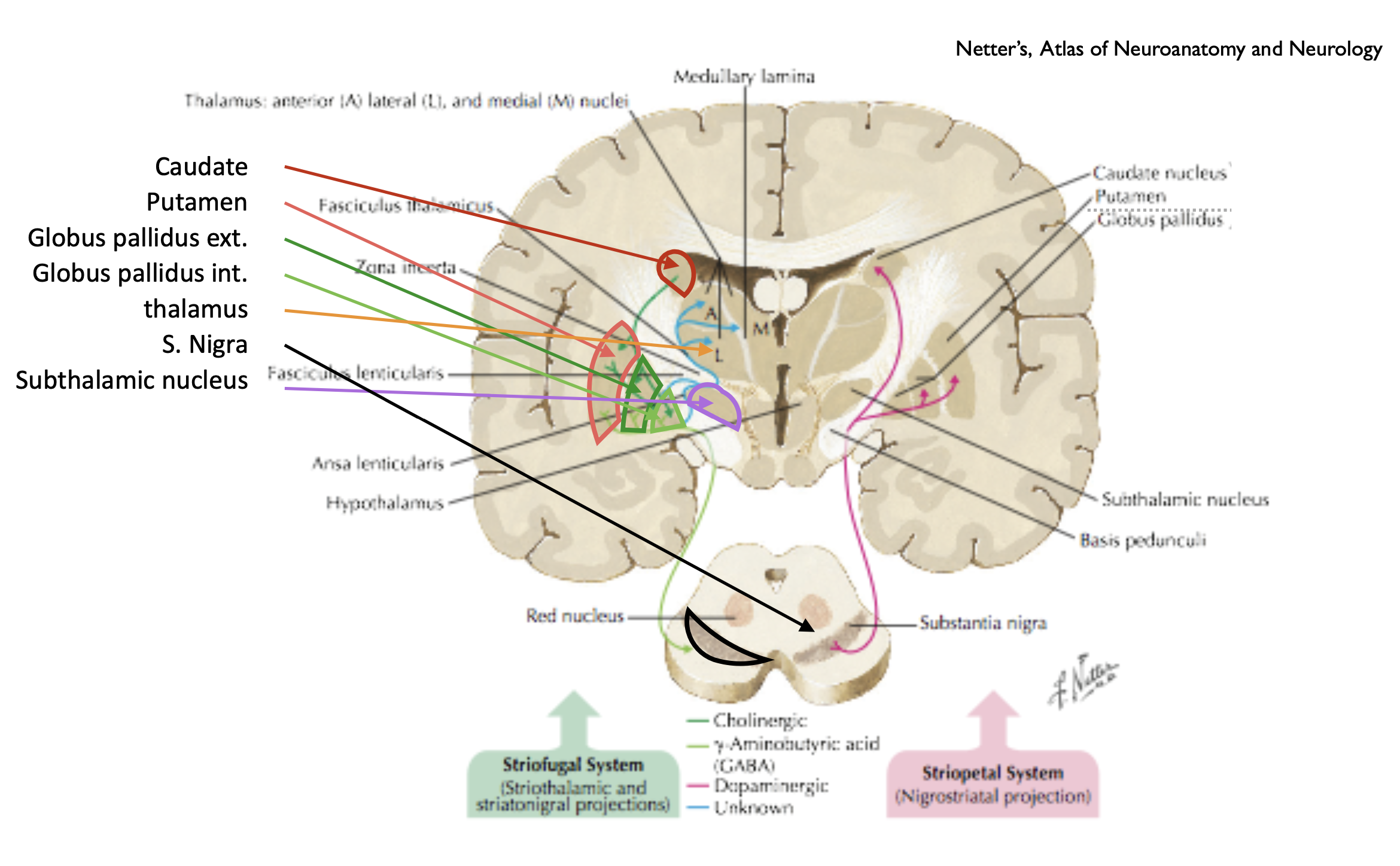
Key Structures to Know Cold
| Structure | Abbreviation | Function in loop |
|---|---|---|
| Caudate + Putamen | Striatum | Main input receiver |
| Nucleus accumbens | Ventral striatum | Reward / motivation input |
| Globus pallidus externus | GPe | Intermediate hub (indirect path) |
| Globus pallidus internus | GPi | Main output nucleus |
| Subthalamic nucleus | STN | Excitatory node in indirect path |
| Substantia nigra pars compacta | SNc | Dopamine source (nigrostriatal tract) |
| Substantia nigra pars reticulata | SNr | Second output nucleus (to brainstem/SC) |
| Thalamus (VA/VL) | Thal | Relay back to cortex |
Anatomical location: between insular cortex and thalamus, with the internal capsule running between the structures.
Discussion Questions
- “The basal ganglia get input from almost the entire cortex. Why do you think that would make evolutionary sense — what kinds of decisions would they need to arbitrate between?”
- “The slide says striatum has ~100 million neurons, but the cortex that projects to it has 16 billion. What does that massive convergence ratio tell you about what the striatum is computing?”
- “The BG are evolutionarily ancient — even lampreys have them (~500 million years old). What does that suggest about what computation they’re doing?”
Common Misconceptions
- “The basal ganglia control movement directly” → Correction: They have mostly indirect influence on muscle activation — they modulate thalamo-cortical activity, not the muscles themselves
- “GPe and GPi are the same” → Correction: GPe is intermediate (in the indirect path); GPi is the final output gate — functionally very different roles
Exam Relevance
- Exam Q3: “How and where are the basal ganglia integrated in the motor system? Name input and output areas.”
- Input: cerebral cortex → striatum; also cortex → STN (hyperdirect)
- Output: GPi/SNr → thalamus (VA/VL) → cortex; SNr also → superior colliculus
4. The Standard Rate Model — The Circuit (20 min)
Core Message
The basal ganglia work by tonic inhibition with selective release. The GPi neurons fire tonically (constantly), holding the thalamus quiet. When a specific movement is selected, the direct pathway briefly silences the GPi, releasing (“disinhibiting”) the thalamus, which then excites the cortex. This is the “gate” model.
⚠️ Fact-check note: The lecture explicitly states this is the “Albin-DeLong Model” and a “simplified explanation that does not adjust well with last year’s research.” Present it as the exam-required framework, but flag that the real picture is more complex.
The Three Pathways
Direct Pathway (facilitatory — 2 inhibitory steps → net disinhibition):
Cortex (Glu+) → Striatum (D1 neurons) (GABA-) → GPi (GABA-) → Thalamus → Cortex
[inhibit] [inhibit] [disinhibited = active]
Net effect: movement facilitation (gate opens)
Indirect Pathway (inhibitory — 3 inhibitory steps → net inhibition):
Cortex (Glu+) → Striatum (D2 neurons) (GABA-) → GPe (GABA-) → STN (Glu+) → GPi (GABA-) → Thalamus → Cortex
[inhibit] [inhibit] [excite] [inhibit] [over-inhibited = silent]
Net effect: movement suppression (gate stays closed)
Hyperdirect Pathway (fastest, most inhibitory — 1 inhibitory step via STN):
Cortex (Glu+) → STN (Glu+) → GPi (GABA-) → Thalamus → Cortex
Net effect: rapid, broad suppression — cancels movements quickly (e.g., “stop!” signal)
Dopamine’s Role
SNc dopaminergic neurons project to the striatum (nigrostriatal tract).
- D1 receptors (on direct pathway neurons): dopamine → activates the direct pathway
- D2 receptors (on indirect pathway neurons): dopamine → inhibits the indirect pathway
- Combined effect: dopamine release = more direct, less indirect = net movement facilitation
Intuitive analogy: Think of dopamine as a bias signal that says “yes, go” — it tips the scales toward action by simultaneously pushing the accelerator (D1) and releasing the brake (D2).
Everyday Analogy for Students
The BG are like a spotlight operator in a theatre. The stage (thalamus/cortex) is normally dark (tonically inhibited by GPi). When a specific actor (movement) needs to perform, the spotlight (direct pathway disinhibition) illuminates exactly that spot — while the rest stays dark (indirect pathway keeps other movements suppressed). The SNc dopamine signal is like the director telling the operator which actor to favor.
Discussion Questions
- “If you had to explain to a first-year student why the direct pathway ‘facilitates’ movement despite having two inhibitory synapses, how would you do it? Walk through it step by step.”
- “Dopamine acts on both D1 and D2 receptors — the same molecule, two opposite effects on the same system. What are the advantages of this design compared to having two separate neurotransmitters?”
- “The hyperdirect pathway is the fastest route and has a net inhibitory effect. When would you need to cancel a movement very quickly? What’s the evolutionary pressure for this?”
Common Misconceptions
- “GABA always inhibits movement” → Correction: GABA inhibiting an inhibitory neuron (GPi) results in excitation downstream — it’s the number of sign-inversions that determines net effect
- “Dopamine excites neurons in the striatum” → Correction: D1 → excitatory effect on direct pathway neurons; D2 → inhibitory effect on indirect pathway neurons — neither is simply “excite the striatum”
- “Direct pathway = direct to muscles” → Correction: “Direct” refers to the shorter route within the BG circuit, not directness to motor output
Exam Relevance
- Exam Q1 (most common): “Make a sketch with all relevant modules and include the neurotransmitters.” — students must know: Glu (cortex→striatum), GABA (striatum→GPi, striatum→GPe, GPe→STN suppression? no: GPe→STN = GABA-), Glu (STN→GPi), GABA (GPi→thalamus)
- Exam Q2: “What happens if the direct or indirect circuit is damaged?” → PD = impaired direct; HD = impaired indirect
5. The BG as Reinforcement Learning System (5 min)
Core Message
The Doya (2000) framework: the brain uses three distinct learning algorithms implemented by different structures.
| Structure | Learning Type | Mechanism |
|---|---|---|
| Cerebellum | Supervised learning | Error signal via climbing fibers |
| Basal ganglia | Reinforcement learning | Dopamine = reward prediction error |
| Neocortex | Unsupervised learning | Self-organization / statistical patterns |
This is a “Most Important Slide” from the lecture — exam-critical.
The BG-dopamine system closely mirrors the Temporal Difference (TD) learning algorithm:
- Dopamine neurons encode reward prediction error (RPE) — firing more than baseline when reward is better than expected, less when worse
- The striatum is the “actor” (selecting actions); the dopamine signal from SNc is the “critic” (evaluating outcomes)
- This is why BG are described as an actor-critic architecture
Striatal subdivisions and learning types:
- Ventral striatum (nucleus accumbens): classical conditioning, motivation, reward
- Dorso-lateral striatum (putamen): habit learning, stimulus-response, well-practiced sequences
- Dorso-medial striatum (caudate): goal-directed learning, novel sequences, outcome-based decisions
Discussion Question
“In the TD learning framework, dopamine encodes reward prediction error — not reward itself. What’s the difference? Can you think of an everyday example where predicting a reward correctly actually reduces the dopamine signal?“
6. Parkinson’s Disease (15 min)
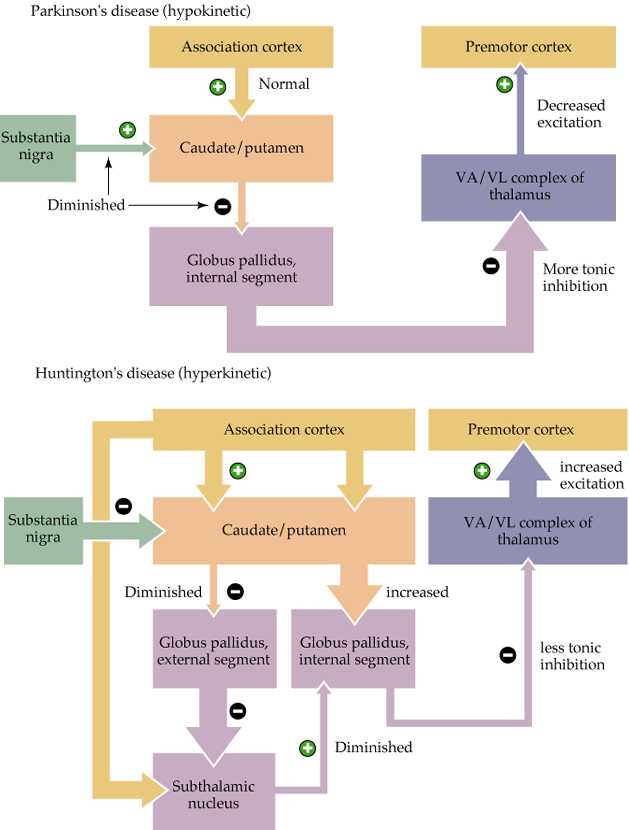
Core Message
PD = loss of dopaminergic neurons in SNc → decreased direct pathway, increased indirect pathway → tonic over-inhibition of thalamus → hypokinesia.
Neuropathology
- Progressive neurodegeneration of SNc dopaminergic neurons
- Symptoms only appear when >60–70% of dopamine neurons have died (massive reserve capacity!)
- Lewy bodies (alpha-synuclein aggregates) found in remaining neurons — pathogenic role unclear
- Prevalence: ~228 per 100,000; second most common neurodegenerative disorder after Alzheimer’s
Three Cardinal Motor Symptoms (exam-required)
- Bradykinesia — slowness and poverty of movement (difficulty initiating and executing)
- Rigidity — increased muscle tone, “cogwheel” resistance
- Resting tremor — 4–6 Hz, pill-rolling, disappears during voluntary movement
⚠️ Fact-check note from vault: The Parkinson’s note lists “involuntary movements of extremities” as a symptom — this is misleading. Resting tremor is the involuntary movement in PD, but the primary deficit is hypokinesia (too little movement). Involuntary movements (dyskinesia) are a side effect of L-DOPA treatment, not a primary symptom of PD. The lecture slides correctly list bradykinesia, tremor, and rigidity as the cardinal triad.
Non-motor symptoms (prodromal and late-stage):
- Hyposmia (loss of smell — often precedes motor symptoms by years)
- Sleep disturbances (RBD)
- Autonomic dysfunction, depression, cognitive decline, dementia
- Timeline: non-motor symptoms begin 2–8 years before motor diagnosis
Treatment
Gold standard: L-DOPA (Levodopa)
- Dopamine cannot cross the blood-brain barrier; L-DOPA (its precursor) can
- Converted to dopamine in the brain, restoring activity toward normal
- Co-administered with DOPA-decarboxylase inhibitors to prevent peripheral conversion and reduce side effects
- Long-term use → dyskinesias (involuntary movements from dopamine overflow in other brain areas)
- Treatment delayed as long as possible; dose must increase over time
Advanced/Surgical:
- DBS (Deep Brain Stimulation) targeting STN or GPi
- Counter-intuitive: stimulation of STN produces therapeutic effect by effectively inhibiting the nucleus (high-frequency stimulation disrupts tonic firing patterns)
- König’s note: “DBS is a big misnomer” — mechanism is not simply stimulation; it likely works through complex network dynamics
- Surgical lesions of STN or GPi (older approach)
Analogy for L-DOPA: Your car’s engine is running on low — L-DOPA is like adding fuel. But if you add too much fuel and the engine floods, you get dyskinesia.
Discussion Questions
- “Symptoms of PD only appear after 60–70% of dopamine neurons have died. What does this extreme reserve capacity tell you about the design of the motor system — is this reassuring or should it concern you from a clinical perspective?”
- “L-DOPA works for years but then leads to dyskinesias. Why would adding dopamine cause unwanted movements if lack of dopamine caused too few movements?”
- “DBS stimulates the STN at high frequency — yet it reduces PD symptoms just like lesioning the STN would. What does that paradox tell you about how the BG circuit might actually be working?”
- “In 1982, six people who used contaminated street drugs developed severe Parkinson’s disease within days — caused by a compound called MPTP. What does this tell us about the cause of PD, and why is MPTP now one of the most used tools in PD research?”
- “Non-motor symptoms like loss of smell and sleep disturbances begin 2–5 years before motor symptoms appear in PD. Why does this window exist, and what’s both the opportunity and the challenge it creates for medicine?”
- “PD cases are projected to increase by 275% between 1990 and 2026 — making it the fastest-growing neurological disorder. What factors could explain this trend, and what does it tell you about the environmental vs. genetic causes of PD?”
Common Misconceptions
- “PD patients can’t move at all” → Correction: They can move, but initiation is severely impaired; interestingly, external visual cues can temporarily bypass the BG gate (patients can step over lines painted on the floor)
- “Parkinson’s is just tremor” → Correction: Tremor is the most visible symptom, but bradykinesia is more disabling and diagnostically primary; cerebellar tremors are intention tremors (worse during movement), PD tremors are resting tremors
7. Huntington’s Disease — Contrast Case (5 min)
Core Message
HD = loss of striatal neurons in the indirect pathway → decreased indirect pathway activity → decreased tonic inhibition of thalamus → hyperkinesia (chorea).
This is the mirror image of Parkinson’s:
| Parkinson’s Disease | Huntington’s Disease | |
|---|---|---|
| Lesion site | SNc dopamine neurons | Striatum (indirect pathway neurons) |
| Affected pathway | Decreased direct pathway | Decreased indirect pathway |
| Net effect on thalamus | Over-inhibited (less movement) | Under-inhibited (more movement) |
| Characteristic movement | Bradykinesia, rigidity, resting tremor | Chorea (involuntary, dance-like movements) |
| Genetics | Mostly idiopathic (environmental + polygenic) | Autosomal dominant (CAG repeat expansion in HTT gene) |
| Prognosis | Not directly fatal | Progressive and fatal |
Early Huntington’s: loss of indirect pathway → direct pathway relatively unopposed → decreased GPi inhibitory output → thalamus over-active → excess movements (chorea)
Late Huntington’s: loss of all striatal neurons → both pathways fail → rigidity develops (similar to late PD)
Discussion Question
“Huntington’s is caused by a known genetic mutation. Given what you know about the BG circuit, could you design a targeted therapy — and at what level of the circuit would you intervene?“
8. Exam Question Round (15 min)
Work through these questions from the lecture’s Questions slide — students answer, you guide.
Question 1: “You find two main pathways from cortex to the basal ganglia. Make a sketch with all relevant modules and include the neurotransmitters.”
Expected key points of a complete answer:
- Direct pathway: Cortex (Glu) → Striatum/D1 (GABA) → GPi (GABA) → Thalamus → Cortex; net disinhibitory
- Indirect pathway: Cortex (Glu) → Striatum/D2 (GABA) → GPe (GABA) → STN (Glu) → GPi (GABA) → Thalamus → Cortex; net inhibitory
- Hyperdirect (bonus): Cortex → STN → GPi → Thalamus; fastest, broadest inhibition
- Dopamine modulation: SNc → Striatum; D1 activates direct, D2 inhibits indirect
Typical mistakes:
- Forgetting the Glu at Cortex → STN (STN is excitatory)
- Getting GPe vs. GPi backwards
- Not mentioning dopamine or the D1/D2 distinction
Question 2: “Which defect is thought to cause Parkinson? Explain the malfunction on the basis of the basal ganglia circuit.”
Expected key points:
- Loss of dopaminergic neurons in SNc
- Less dopamine → less direct pathway activation (D1) + less indirect pathway inhibition (D2)
- Net: increased GPi activity → more tonic inhibition of thalamus → less cortical activation → bradykinesia/rigidity
-
60–70% neuron loss required before symptoms appear
- Note: this is a simplified explanation — lecture explicitly states it doesn’t fully explain recent findings
Typical mistakes:
- Saying “dopamine loss = less movement” without explaining the circuit mechanism
- Not mentioning tonic inhibition of thalamus as the key bottleneck
- Mixing up the direction: less dopamine does NOT mean less indirect pathway activity — it means LESS suppression of indirect pathway → MORE indirect activity
Question 3: “Compare lesions and symptoms of Morbus Parkinson and Chorea Huntington.”
Expected key points:
- PD: SNc degeneration → decreased direct, increased indirect → tonic over-inhibition → hypokinesia
- HD: striatal degeneration (indirect pathway neurons) → decreased indirect → reduced inhibition → hyperkinesia (chorea)
- Contrast: PD = too much inhibition of thalamus; HD = too little
- Bonus: early HD mimics dopamine excess; late HD converges toward a PD-like state
Typical mistakes:
- Saying HD damages the direct pathway (it’s primarily the indirect pathway neurons that are lost early)
- Not explaining the circuit mechanism — just listing symptoms without connecting to BG pathology
Closing (3 min)
Take-Home Message:
“The basal ganglia are not a movement generator — they are a movement selector. They work by keeping everything tonically inhibited and selectively releasing specific actions via a dopamine-modulated gate. When the dopamine signal breaks down, the gate stays closed (Parkinson’s); when the brake of the indirect pathway is lost, the gate can’t close properly (Huntington’s).”
Preview of next week — Lecture 4: Motor Cortex:
If the BG decide which movement to permit, the motor cortex is where the movement plan is actually encoded and executed. Next week we look at population coding (Georgopoulos), the motor homunculus, and how single neurons can represent movement direction through cosine tuning — and what happens when we read those signals out in BCIs.
Quick Reference: Neurotransmitter Summary
| Synapse | Neurotransmitter | Effect |
|---|---|---|
| Cortex → Striatum | Glutamate | Excitatory |
| Cortex → STN (hyperdirect) | Glutamate | Excitatory |
| Striatum (D1) → GPi | GABA | Inhibitory |
| Striatum (D2) → GPe | GABA | Inhibitory |
| GPe → STN | GABA | Inhibitory |
| STN → GPi | Glutamate | Excitatory |
| GPi → Thalamus | GABA | Tonic inhibitory |
| Thalamus → Cortex | Glutamate | Excitatory |
| SNc → Striatum (D1) | Dopamine | Excitatory (via D1) |
| SNc → Striatum (D2) | Dopamine | Inhibitory (via D2) |